The ending of that realclearpolitics article. I think this is the beginning of the end for the obstructionists. They should be afraid - does the publisher of WaPo or the CEO of twitter have any background in medicine and virology? They should worry - helping stop an important treatment during a brutal pandemic.... could turn into a serious liability. It probably will.
In reality just the opposite was true. This was a tragic mistake by Fauci and FDA Commissioner Dr. Stephen Hahn and it was a mistake that would cost the lives of thousands of Americans in the days to come.
At the same time, accumulating data showed remarkable results if hydroxychloroquine were given to patients early, during a seven-day window from the time of first symptom onset. If given during this window, most infections did not progress into the severe, lethal second stage of the disease. Patients still got sick, but they avoided hospitalization or the later transfer to an intensive care unit. In mid-April a high-level memo was sent to the FDA alerting them to the fact that the best use for hydroxychloroquine was for its early use in still ambulatory COVID patients. These patients were quarantined at home but were not short of breath and did not yet require supplemental oxygen and hospitalization.
Failing to understand that COVID-19 could be a two-stage disease process, the FDA ignored the memo and, as previously mentioned, it withdrew its EUA for hydroxychloroquine based on flawed studies and clinical trials that were applicable only to late-stage COVID patients.
By now, however, some countries had already implemented early, aggressive, outpatient community treatment with hydroxychloroquine and within weeks were able to minimize their COVID deaths and bring their national pandemic under some degree of control.
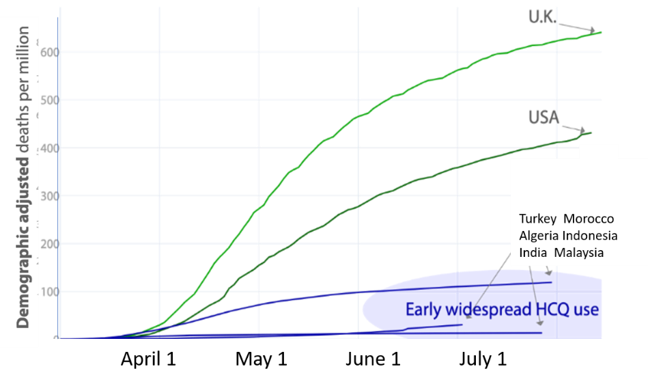
In countries such as Great Britain and the United States, where the “Fauci-Hahn Strategy” was followed, there was a much higher death rate and an ever-increasing number of cases. COVID patients in the U.S. would continue to be quarantined at home and left untreated until they developed shortness of breath. Then they would be admitted to the hospital and given hydroxychloroquine outside the narrow window for the drug’s maximum effectiveness.
In further contrast, countries that started out with the “Fauci-Hahn Doctrine” and then later shifted their policy towards aggressive outpatient hydroxychloroquine use, after a brief lag period also saw a stunning rapid reduction in COVID mortality and hospital admissions.
Finally, several nations that had started using an aggressive early-use outpatient policy for hydroxychloroquine, including France and Switzerland, stopped this practice when the WHO temporarily withdrew its support for the drug. Five days after the publication of the fake Lancet study and the resulting media onslaught, Swiss politicians banned hydroxychloroquine use in the country from May 27 until June 11, when it was quickly reinstated.

The consequences of suddenly stopping hydroxychloroquine can be seen by examining a graph of the Case Fatality Ratio Index (nrCFR) for Switzerland. This is derived by dividing the number of daily new COVID fatalities by the new cases resolved over a period with a seven-day moving average. Looking at the evolution curve of the CFR it can be seen that during the weeks preceding the ban on hydroxychloroquine, the nrCFR index fluctuated between 3% and 5%.
Following a lag of 13 days after stopping outpatient hydroxychloroquine use, the country’s COVID-19 deaths increased four-fold and the nrCFR index stayed elevated at the highest level it had been since early in the COVID pandemic, oscillating at over 10%-15%. Early outpatient hydroxychloroquine was restarted June 11 but the four-fold “wave of excess lethality” lasted until June 22, after which the nrCFR rapidly returned to its background value.
Here in our country, Fauci continued to ignore the ever accumulating and remarkable early-use data on hydroxychloroquine and he became focused on a new antiviral compound named remdesivir. This was an experimental drug that had to be given intravenously every day for five days. It was never suitable for major widespread outpatient or at-home use as part of a national pandemic plan. We now know now that remdesivir has no effect on overall COVID patient mortality and it costs thousands of dollars per patient.
Hydroxychloroquine, by contrast, costs 60 cents a tablet, it can be taken at home, it fits in with the national pandemic plan for respiratory viruses, and a course of therapy simply requires swallowing three tablets in the first 24 hours followed by one tablet every 12 hours for five days.
There are now 53 studies that show positive results of hydroxychloroquine in COVID infections. There are 14 global studies that show neutral or negative results -- and 10 of them were of patients in very late stages of COVID-19, where no antiviral drug can be expected to have much effect. Of the remaining four studies, two come from the same University of Minnesota author. The other two are from the faulty Brazil paper, which should be retracted, and the fake Lancet paper, which was.
Millions of people are taking or have taken hydroxychloroquine in nations that have managed to get their national pandemic under some degree of control. Two recent, large, early-use clinical trials have been conducted by the Henry Ford Health System and at Mount Sinai showing a 51% and 47% lower mortality, respectively, in hospitalized patients given hydroxychloroquine. A recent study from Spain published on July 29, two days before Margaret Sullivan’s strafing of “fringe doctors,” shows a 66% reduction in COVID mortality in patients taking hydroxychloroquine. No serious side effects were reported in these studies and no epidemic of heartbeat abnormalities.
This is ground-shaking news. Why is it not being widely reported? Why is the American media trying to run the U.S. pandemic response with its own misinformation?
Steven Hatfill is a veteran virologist who helped establish the Rapid Hemorrhagic Fever Response Teams for the National Medical Disaster Unit in Kenya, Africa. He is an adjunct assistant professor in two departments at the George Washington University Medical Center where he teaches mass casualty medicine. He is principle author of the prophetic book “Three Seconds Until Midnight -- Preparing for the Next Pandemic,” published by Amazon in 2019.
|



